
"Chemical peel" is one of the most searched skincare treatments — and one of the most misunderstood. Some people picture an aggressive "skin-stripping" procedure that leaves the face raw and fragile; others expect a single session to erase everything from acne to melasma. Neither picture is accurate.
In reality, chemical peeling is a dermatologic procedure that has been performed for more than 50 years with an excellent safety record when done properly by trained professionals. Prescribed correctly, peels improve acne, post-acne dark marks, rough dull texture and certain pigment concerns. Done wrong — wrong acid, wrong strength, wrong skin type, wrong timing — a peel can cause lasting dark patches, irritation or even scarring.
This guide covers everything you need to know: what a chemical peel actually is, how it works, the different types, who should (and shouldn't) get one, what a medically supervised session looks like, and how to care for your skin afterward. It is based on guidance from the American Academy of Dermatology (AAD), Cleveland Clinic, DermNet and peer-reviewed dermatology references, combined with real treatment experience at Eternal Beauty Center, a skin clinic in Go Vap, Ho Chi Minh City.
1. What is a chemical peel?
A chemical peel is a procedure in which a solution — usually one or more acids at a carefully controlled concentration — is applied to the skin to deliberately remove old, damaged layers of skin cells, prompting the skin to regenerate a fresher, healthier, more even-toned surface.
Think of it this way: your skin renews itself constantly, shedding old surface cells to make room for younger cells underneath. That cycle slows with age and gets "clogged up" by oil, acne and sun damage. A chemical peel accelerates the renewal cycle in a controlled way — the practitioner intentionally creates a shallow injury at a precise depth, and the skin repairs itself with a new surface.
The key word is controlled: the choice of acid, its concentration, how long it stays on the skin and how deep it acts are all calibrated to your specific skin condition. That is why chemical peeling is classified as a medical procedure, not a casual at-home skincare step.
A note on terminology: in the beauty market, "peel" is sometimes used loosely for ordinary exfoliating facials. In this article, we mean the dermatologic definition: a resurfacing treatment using treatment-strength actives, performed at a qualified clinic.
2. How peels work: why controlled exfoliation improves skin

When the peel solution touches the skin, the active ingredients break the bonds holding old, keratinized surface cells together, causing them to shed — sometimes visibly, sometimes microscopically. That triggers a cascade of benefits:
A renewed surface: dull, rough dead-cell buildup is cleared away, leaving skin brighter and smoother.
Unclogged pores: oil-soluble BHA (salicylic acid) peels travel into the follicle itself, dissolving sebum and comedones — which is why peels are a core tool in acne treatment.
Regeneration signals: the controlled injury activates the skin's repair response, stimulating new cell turnover and, with deeper peels, collagen production.
More even tone: peels help disperse and shed excess melanin trapped in the epidermis — the main mechanism behind their effect on post-acne marks and superficial pigmentation.
How strongly each benefit shows up depends directly on peel depth — the subject of the next section.
3. The three peel depths: superficial, medium and deep
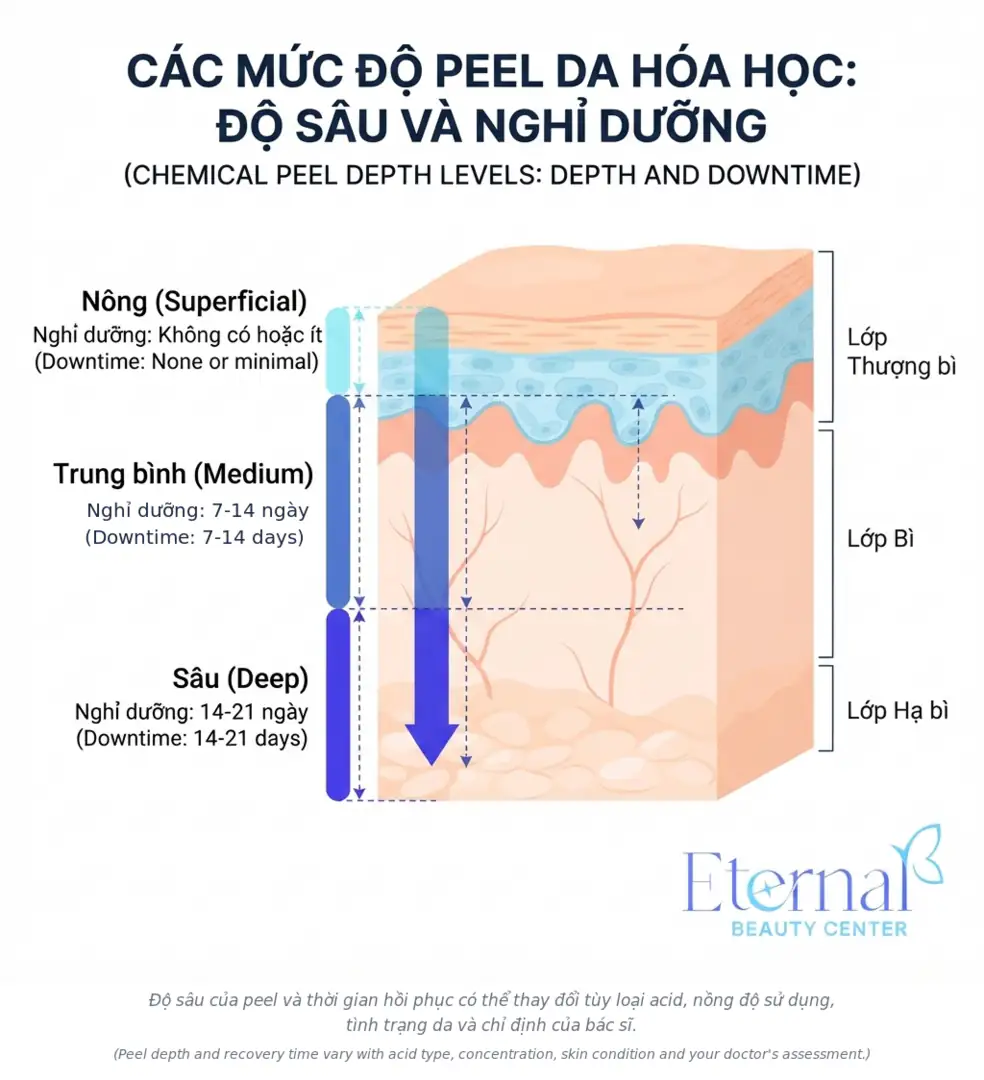
Dermatology classifies peels by how deep they act in the skin. This is the single most important classification — it determines results, downtime and risk.
| Superficial peel | Medium peel | Deep peel | |
|---|---|---|---|
| Depth | Epidermis | Epidermis + upper dermis | Deep dermis |
| Typical agents | Glycolic, salicylic, lactic, mandelic, light Jessner | TCA 20–35%, Jessner + TCA | Phenol |
| Sensation | Mild tingling for a few minutes | Distinct burning, needs soothing | Painful, requires anesthesia |
| Downtime | Little to none (0–3 days) | 7–14 days (redness, swelling, crusting) | 2–3 weeks or more |
| Sessions usually needed | 3–6, spaced 2–5 weeks apart | 1–2 per year | Once in a lifetime |
| Best for | Acne, mild dark marks, dull rough skin | Superficial pigment, shallow acne scars, fine lines | Deep wrinkles, severe damage (rarely used) |
Three things worth remembering:
Superficial peels — the everyday "lunchtime peel"
These make up the vast majority of peels performed in skin clinics, and they suit the most common goals: acne, oily skin, mild dark marks and uneven tone. Because they act only on the epidermis, downtime is minimal — many modern superficial peel systems cause no visible flaking at all. The trade-off: results build gradually and require a course of several sessions (typically 3–6) rather than a single visit.
Medium peels — stronger results, real downtime
Usually trichloroacetic acid (TCA) at 20–35%, reaching the upper dermis. They deliver more visible improvement for pigmentation, shallow acne scarring and fine lines, but expect redness, swelling and crusting for one to two weeks. Medium peels demand an experienced physician — especially on Asian skin, which is prone to post-inflammatory hyperpigmentation.
Deep peels — rarely recommended today
Phenol peels reach the deep dermis and can dramatically improve severe wrinkling, but they are rarely used nowadays because of toxicity concerns, scarring risk, permanent pigment loss, and the need for anesthesia and cardiac monitoring. For Asian skin tones, deep peels are almost never advised.
4. Common peeling agents

Each acid has its own "personality" — knowing them makes conversations with your dermatologist much easier:
AHAs (alpha hydroxy acids) — glycolic, lactic, mandelic
Water-soluble acids derived from sugar cane, milk and almonds. Glycolic acid is the classic AHA: a small molecule that penetrates quickly, effective for dullness, rough texture and mild dark marks. Lactic and mandelic acids have larger molecules, act more gently, and are safer choices for sensitive and darker skin.
BHA (beta hydroxy acid) — salicylic acid
Oil-soluble, so it travels deep into the follicle — the go-to active for oily skin, blackheads and closed comedones. Salicylic acid is also mildly anti-inflammatory, helping calm inflamed breakouts. If you're researching peels for acne, your protocol will almost certainly include BHA.
TCA (trichloroacetic acid)
The most versatile agent: low concentrations for superficial peels, 20–35% for medium-depth peels. At very high concentrations, TCA is also applied dot by dot into individual scar pits in the TCA Cross technique for atrophic acne scar treatment — a completely different application from a full-face peel, strictly physician-performed.
Retinol / retinoic acid (the "yellow peel")
Vitamin A derivatives, nicknamed for the solution's yellow color. They accelerate cell turnover and help with acne, dark marks and early signs of aging, typically with light flaking for a few days. Not for use during pregnancy or breastfeeding.
Jessner's solution and combination formulas
The classic Jessner's solution combines salicylic acid, lactic acid and resorcinol — often used to boost results for oily, acne-prone skin or to "prime" the skin before TCA. Modern peel systems frequently blend several acids at moderate strengths with soothing agents, delivering solid results without dramatic visible peeling — practical if you need to go to work or school right after your session.
Next-generation resorcinol derivatives
Refined resorcinol derivatives are used in advanced pigment protocols that reach melanin in deeper layers without heat — the approach behind modern resistant-melasma treatment protocols.
5. What can a chemical peel actually improve?

Result after one Acne Peel session — actual outcomes vary with each person’s skin condition.
According to Cleveland Clinic and the AAD, peels are indicated for a fairly wide range of concerns — but they work best on problems located in the superficial layers of the skin:
Acne: BHA/AHA peels unclog follicles, reduce comedones and help calm inflammation; they're usually combined with medical-grade acne extraction in a complete treatment plan. For closed comedones — the stubborn "hidden acne" that rarely clears on its own — peels are among the most-used solutions (see: Does hidden acne go away on its own?).
Post-acne dark marks (PIH): peels speed up the shedding of pigment left behind after breakouts, fading marks noticeably faster than waiting them out. Read more about how these marks form in Why do dark marks appear after acne?.
Superficial melasma and uneven tone: peels can help epidermal melasma and light freckling; melasma, however, is a complex chronic pigment disorder that usually needs a multi-modality plan — a peel alone is rarely enough (see: Melasma: causes and treatment).
Dull, rough skin and enlarged-looking pores: clearing thickened dead-cell buildup leaves skin smoother, brighter and better able to absorb skincare.
Early photoaging: fine lines and rough, dry texture from accumulated sun damage.
Shallow acne scars: medium peels can soften very shallow scarring; true atrophic scars need dedicated techniques such as TCA Cross, subcision and microneedling (see The 3 types of atrophic acne scars).
What peels can NOT fix: deep atrophic scars, deep wrinkles, skin laxity, visible capillaries — and they don't replace medical treatment for active skin disease. Setting the right expectations up front is what determines whether you'll be happy with your peel.
6. Who is (and isn't) a good candidate?
Good candidates
Oily skin, comedonal or mildly inflamed acne, blackheads, closed comedones
Post-acne dark marks, uneven or dull skin tone
Rough texture, enlarged-looking pores
Early signs of aging; anyone wanting overall brightness and smoothness
Proceed with caution — or postpone
Pregnancy and breastfeeding: several peel actives (retinoids and high-strength salicylic acid in particular) are not recommended.
Current isotretinoin use, or recently stopped without the washout period your doctor requires.
Open wounds, active infection, eczema, psoriasis or an active herpes outbreak in the treatment area; severely inflamed acne should be brought under control first.
History of keloid or hypertrophic scarring: higher risk of scarring after any resurfacing procedure.
Recent intense sun exposure or sunburn, or inability to commit to strict sun protection afterward.
Unrealistic expectations: hoping for "instantly whiter skin" or scar removal from a peel alone.
Most Vietnamese and other Southeast Asian skin falls into Fitzpatrick types III–IV — skin that develops post-inflammatory hyperpigmentation (PIH) more readily than fair skin. Per DermNet, these skin types can absolutely be peeled, but they call for a practitioner experienced with darker skin, a preference for gentle superficial agents, and sometimes a "skin-priming" phase with pigment-suppressing actives before the first peel. This is exactly why the pre-peel consultation and skin analysis matter as much as the peel itself.
7. What a medically supervised peel session looks like
A superficial peel at a medically run clinic typically takes 45–90 minutes:
1. Consultation and skin analysis: the doctor assesses your skin condition, acne/pigment type, allergy history and current medications to choose the right agent and strength — or advises against peeling if your skin isn't ready.
2. Deep cleansing: makeup removal, cleansing and degreasing so the solution absorbs evenly.
3. Protecting sensitive areas: the corners of the eyes, nose and mouth are shielded.
4. Applying the peel: layer by layer, with the skin's reaction monitored continuously. A few minutes of tingling or mild warmth is normal.
5. Neutralizing and soothing: depending on the system, the solution is neutralized at the right moment, followed by calming, restorative care.
6. Sunscreen + instructions: sunscreen is applied, home-care instructions given, and your next session scheduled.
In comprehensive acne protocols, the peel is often just one link in a full treatment session — cleansing, extraction, peel, anti-inflammatory care and recovery — the way E-Acne, our medical acne treatment, is structured.
8. Post-peel skincare

Peel results depend 50% on the session, 50% on what you do afterward. The core rules, per the AAD:
Strict sun protection — rule number one. Post-peel skin is more UV-sensitive than usual; skip sunscreen and you don't just lose your results — you can end up darker than before the peel. Use a broad-spectrum SPF 30+ daily and cover up outdoors (full guide: Sun protection done right).
Never pick, scratch or rub flaking skin. Peeling off healing skin is the fastest route to dark marks and scars.
Moisturize consistently with the gentle, restorative products you're instructed to use; well-hydrated skin sheds evenly and heals faster.
Pause strong actives (retinoids, at-home AHA/BHA, scrubs) until the skin has fully recovered — usually 5–7 days for a superficial peel.
Cleanse gently with a mild cleanser and cool or lukewarm water; avoid saunas, swimming pools and sweaty workouts for the first few days.
Watch for warning signs: increasing pain, significant swelling, spreading blisters or signs of infection — contact your clinic immediately.
Note: not every peel causes visible flaking. Many modern superficial peel systems shed cells only microscopically — your skin gradually brightens without a "snake-shedding" phase. More flaking does not mean better results.
9. Are chemical peels safe? Risks for Asian skin tones
According to the AAD, dermatologists have performed chemical peels for over 50 years with an excellent safety record. But "safe" always comes with conditions: right indication, right technique, right aftercare. Possible risks include:
Irritation and prolonged redness — the most common issue; usually mild and self-resolving.
Post-inflammatory hyperpigmentation (PIH): the most relevant risk for Asian skin. An overly aggressive peel, unprepped skin or sun exposure afterward can all leave skin darker than it started.
Hypopigmentation and scarring: rare; mostly associated with medium/deep peels or poor technique.
Herpes (cold sore) reactivation in people with a history — one more reason full disclosure at consultation matters.
Infection: rare, usually linked to improper aftercare.
What about at-home peels?
High-strength "at-home peel" products sold widely online are a genuine concern: unverified concentrations, no skin assessment beforehand, and nobody to neutralize the acid or manage a strong reaction. A large share of the burns and pigment damage that skin clinics see walk in the door started with a high-strength home peel. If you want to use acids at home, stay at cosmetic strengths (e.g. 1–2% BHA, under 10% AHA) and get professional advice; leave treatment-strength peels to a physician.
10. 5 common myths about chemical peels
1. "Peels thin out and erode your skin." A properly performed peel removes only the old, expendable layer of dead surface cells and stimulates new cell renewal. Thin, fragile skin is the consequence of peeling done wrong — too frequent, too strong — not of peeling itself.
2. "The more you flake, the better it's working." False. Visible flaking reflects the depth of action, not the quality of results. Many no-flake peel systems deliver clear improvement over a course of sessions.
3. "One peel and your skin is instantly bright and flawless." Superficial peels need a course of 3–6 sessions for visible change; results build gradually. A clinic promising "one shade lighter after one peel" is a red flag.
4. "Peels cure melasma for good." Melasma is a chronic, multi-mechanism pigment disorder; a peel is one supporting tool within a broader protocol, and melasma can always recur without diligent sun protection and maintenance.
5. "Every skin type gets the same peel." Every skin — especially darker, sensitive or inflamed skin — needs its own agent, concentration and schedule. A personalized protocol is the standard of care, not an upgrade.
11. Chemical peels at Eternal Beauty Center

At Eternal Beauty Center in Go Vap, Ho Chi Minh City, peels are never sold as a one-formula-fits-all service — every client gets a dermatologist consultation and skin analysis before any peel is prescribed:
Acne Peel — a dedicated protocol for oily, acne-prone skin: deep cleansing, comedone clearance and an acne-appropriate peel to clear stubborn breakouts and rebalance oil. Learn more in Acne Peel at Eternal — deep care for inflamed acne-prone skin.
Mela Peel — post-acne pigmentation peel: a personalized peel for red and brown post-acne marks (PIH), designed to involve no visible flaking and no downtime — practical for busy schedules.
Eternal Peel — a gentle peel without peeling: surface renewal for dull, rough, uneven-toned skin with immediate brightness and smoothness.
E-Acne — medical acne treatment: a dermatologist-led comprehensive protocol in which the peel is one coordinated step alongside extraction and recovery care.
E-Mela — resistant melasma treatment: an advanced pigment protocol using next-generation resorcinol derivatives to reach deeper pigment without heat, non-invasively.
Every treatment course includes detailed post-peel care instructions and follow-up visits so the doctor can track how your skin responds session by session.
12. Frequently asked questions
How often can you get a chemical peel?
For superficial peels, sessions are usually spaced 2–5 weeks apart, with a typical course of 3–6 sessions. Medium peels should only be done once or twice a year. Your exact schedule should be set by a doctor based on your skin's response.
Do chemical peels hurt?
Superficial peels cause only tingling and mild warmth for a few minutes before settling. Medium peels sting more noticeably and need soothing measures. Severe or persistent pain is not normal — tell your practitioner immediately.
Will my skin flake afterward? If it doesn't, did the peel fail?
It depends on the peel system: some cause light flaking for a few days, others shed cells only microscopically. The amount of visible flaking does not correlate with effectiveness — many no-flake systems show clear results over a full course.
How soon can I wear makeup again?
After a no-flake superficial peel, light makeup is usually fine after 24–48 hours if there's no irritation. If your skin is flaking or still red, wait until it has fully healed — and always follow your clinic's specific instructions.
Can a chemical peel treat melasma?
Peels can support improvement of superficial melasma and uneven tone, but melasma is a chronic, multi-mechanism condition that needs a combined protocol and strict ongoing sun protection. No method — peels included — cures melasma "permanently."
Can sensitive or darker skin be peeled?
Yes, with gentler acids (lactic, mandelic), lower concentrations, and a practitioner experienced with darker skin, since the risk of post-inflammatory hyperpigmentation is higher. A pre-peel consultation is essential.
Can I get a peel while pregnant?
Several peel actives (retinoids and high-strength salicylic acid in particular) are not recommended during pregnancy or breastfeeding. Tell your doctor so they can suggest safe alternatives for your skin.
Can I do a peel at home?
Not at treatment strengths. If you want to use acids at home, stay within cosmetic concentrations (1–2% BHA, under 10% AHA) — and leave stronger peels to a physician. DIY treatment-strength peels are a leading cause of burns and pigment damage.
13. Key takeaways
A chemical peel is a controlled removal of old, damaged skin layers using treatment-strength actives to trigger renewal — a tool dermatology has relied on for over 50 years. The essentials:
Peels come in three depths — superficial, medium, deep; everyday goals (acne, dark marks, dullness) are addressed mainly with superficial peels over a multi-session course.
Realistic benefits: better acne control, faster-fading post-acne marks, smoother brighter texture, support for superficial pigment concerns. Peels do not fix deep scars, deep wrinkles or cure melasma.
Vietnamese and other Asian skin (Fitzpatrick III–IV) is PIH-prone — choose a clinic with physician oversight and a personalized protocol.
Sunscreen and hands-off healing are the two non-negotiables after any peel.
More flaking ≠ better results; realistic expectations are the foundation of a good outcome.
Book a skin analysis & peel consultation at Eternal Beauty Center
Not sure which peel suits your skin — or tried peels before without seeing results? The dermatology team at Eternal Beauty Center will analyze your skin, assess your acne, marks and pigment condition, and design a personalized peel protocol for you.
Hotline / Zalo / WhatsApp: +84 334 713 610
Address: 204 Street No. 1, Ward 16, Go Vap District, Ho Chi Minh City
Opening hours: 10:00 AM – 8:00 PM daily
Explore our peel services: Acne Peel · Mela Peel · Eternal Peel
Medical disclaimer: This article is for informational purposes only and does not replace an in-person examination, diagnosis or personalized medical advice. Chemical peeling is a procedure that must be prescribed and performed by qualified professionals; suitability and results vary from person to person. Please consult a dermatologist before undergoing any peel.


