Melasma is one of the most common — and most stubborn — pigment problems among Vietnamese women, especially after pregnancy and after the age of 30. In this article, Dr. Le Hien explains what melasma actually is, why it appears, which treatments are backed by evidence, and why melasma can almost never be "cured once and gone forever".
Medical note: This article is for information only and does not replace an in-person consultation and diagnosis. Melasma comes in several forms and is easily confused with other pigment disorders; the right protocol must be personalized by a dermatologist after a skin assessment.
What is melasma?
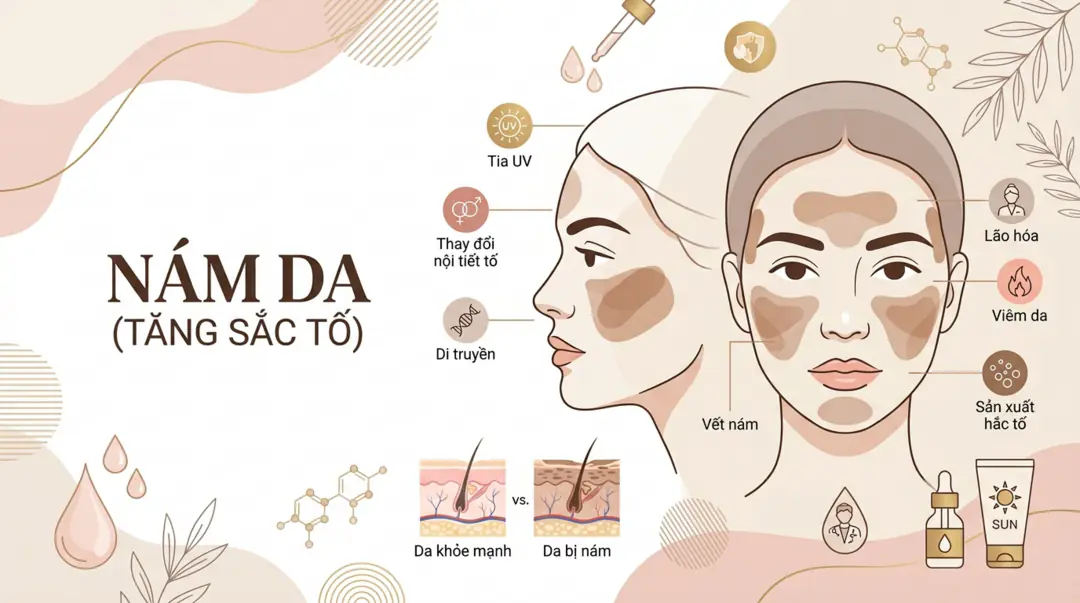
Melasma (formerly called chloasma or the "mask of pregnancy") is an acquired form of hyperpigmentation that shows up as brown to grey-brown patches, symmetrical on both sides of the face, with irregular borders. The most common locations are the cheeks, forehead, bridge of the nose, and upper lip — a centrofacial pattern seen in 50–80% of cases.
At its core, melasma develops when pigment cells (melanocytes) become overactive and produce more melanin than usual. It is not dangerous to your health and it is not contagious, but it has a real impact on appearance and confidence.
One thing to understand from the start: melasma is a chronic, relapse-prone condition. A realistic treatment goal is to fade, control, and maintain — not to "erase it permanently".
Melasma vs. freckles vs. post-acne marks
This is the step people get wrong most often, and that mistake leads to choosing the wrong treatment.
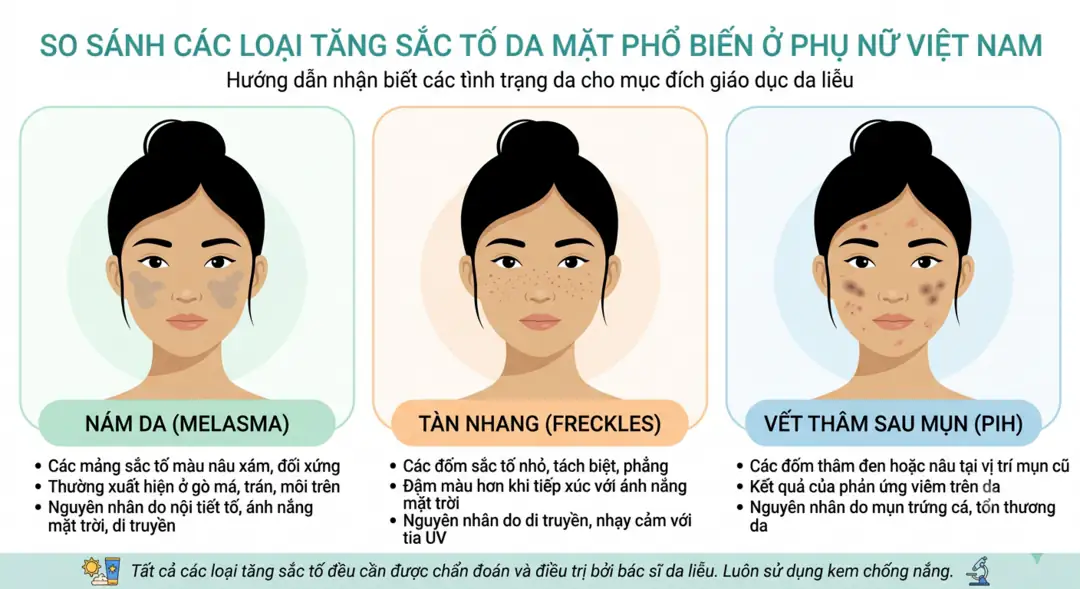
Melasma: symmetrical brown/grey-brown patches with soft borders, spreading across the cheeks, forehead, and upper lip. Darkens noticeably with sun exposure, pregnancy, or hormonal therapy. Strongly linked to hormones and UV.
Freckles: small, round, light-to-dark brown spots that appear individually rather than as patches. They usually show up early in life, have a clear genetic component, and darken in summer.
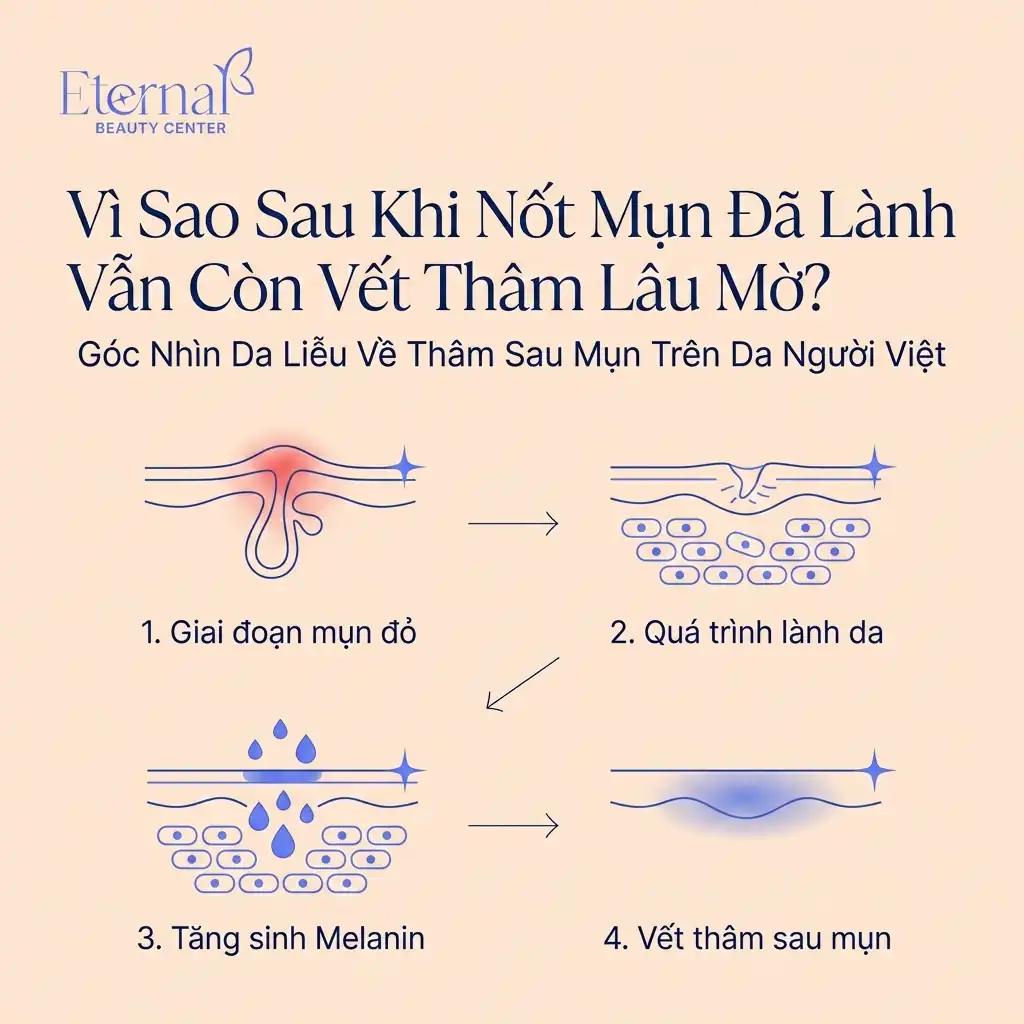
Post-inflammatory hyperpigmentation (PIH / post-acne marks): dark marks left exactly where a pimple or inflammatory lesion used to be. They have sharper borders than melasma and often fade over time with good sun protection. This is a different problem with its own approach — see the Mela Peel service designed for post-acne marks.
| Criteria | Melasma | Freckles | Post-acne marks (PIH) |
|---|---|---|---|
| Appearance | Patches, symmetrical | Small separate spots | Marks where acne used to be |
| Borders | Soft | Defined | Fairly defined |
| Main driver | Hormones + UV | Genetics | Prior inflammation/acne |
| Course | Chronic, relapse-prone | Stable | Usually fades over time |
Accurate distinction requires a dermatologist’s skin assessment, because many people have both melasma and post-acne marks at the same time, which calls for a combined protocol.
The three types of melasma and how well they respond
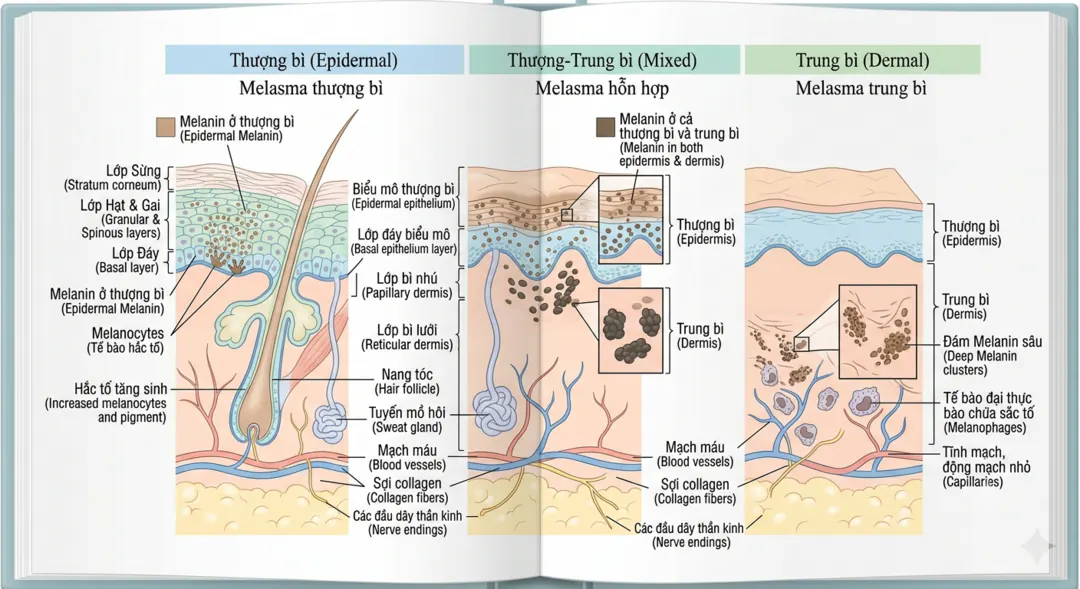
Based on how deep the pigment sits in the skin, melasma is divided into three types — and this is what determines whether your melasma is "easy" or "hard" to treat:
Epidermal melasma: pigment sits in the shallow layer. Dark brown, well-defined patches. Responds best to treatment.
Dermal melasma: pigment sits deeper. Light brown to blue-grey, blurred borders. Responds poorly and is hard to fully clear.
Mixed melasma: a combination of both — and the most common type. Usually improves partially and needs patience.
| Melasma type | Pigment depth | Treatment response |
|---|---|---|
| Epidermal | Shallow | Best |
| Dermal | Deep | Poor |
| Mixed | Both | Partial improvement (most common) |
This is why two people who both "have melasma" can get very different results. There is no one-size-fits-all protocol.
Causes and risk factors

Melasma results from several overlapping factors, not a single cause:
Genetics. Around 60% of people with melasma have an affected family member. Genetic predisposition sets the stage.
UV light — and visible light too. This is the strongest trigger and aggravator. UV stimulates melanocytes to produce more melanin. Importantly, visible light (including blue light) from the sun — and partly from screens — can also darken melasma, especially in deeper skin tones.
Hormones. Pregnancy, oral contraceptives, and hormone replacement therapy can all trigger melasma. This is why melasma so often appears after childbirth and earns the nickname "mask of pregnancy".
Certain medications and cosmetics. Some photosensitizing medications, along with irritating cosmetics, can help trigger or sustain melasma.
Heat and inflammation. High heat and heat-generating procedures (such as some unsuitable lasers/IPL) can stimulate melanocytes and make melasma worse.
Why Vietnamese women are prone to melasma
Most Vietnamese women fall into Fitzpatrick skin types III–IV — the group most prone to pigmentation. Add a hot, sunny climate year-round, high UV intensity, and often inconsistent sun protection, and melasma becomes very common in the 30–50 age range.
Post-pregnancy hormonal shifts, the cultural pressure to be fair-skinned, and the habit of buying unregulated "whitening" or anti-melasma creams make things even more complicated.
How melasma is diagnosed at a dermatology clinic

A proper melasma exam goes beyond the naked eye. A dermatologist typically:
Takes a history: when it started, any link to pregnancy/hormones, past cream use, sun exposure.
Examines the skin with a Wood’s lamp: helps estimate pigment depth (epidermal vs. dermal) and therefore the likely response.
Distinguishes it from other pigment disorders such as freckles, sun spots, or post-inflammatory hyperpigmentation.
This diagnostic step shapes the entire protocol. Skipping it — as happens when people buy creams on a tip — is a common reason treatment fails.
Evidence-based medical treatments for melasma
Effective melasma treatment is always a layered combination, with sun protection as the non-negotiable foundation.
Sun protection — the essential foundation

No step matters more than sun protection. Per dermatology society guidance, people with melasma should:
Use a broad-spectrum sunscreen, SPF 30 or higher, ideally mineral-based (zinc oxide, titanium dioxide) and especially containing iron oxide, which helps block visible light. Tinted sunscreens usually contain iron oxide.
Reapply every 2–3 hours when outdoors.
Add a wide-brimmed hat, mask, sunglasses, and seek shade.
Without serious, year-round sun protection, every other treatment is nearly meaningless.
Topical treatments

Hydroquinone: the "gold standard" for lightening melasma, but used only under a doctor’s prescription and supervision, for a limited course, to avoid side effects.
Triple combination: hydroquinone + tretinoin + a mild corticosteroid, reported to improve 60–80% of cases. This is a prescription protocol, not for unsupervised long-term use.
Gentler actives: azelaic acid, kojic acid, vitamin C, niacinamide — suitable for maintenance or for those who cannot use hydroquinone.
Thiamidol: a newer-generation tyrosinase inhibitor that, in several recent studies, reduced melasma severity with little irritation.
Tranexamic acid
Tranexamic acid (oral or topical) is considered an option for stubborn, treatment-resistant melasma and must be prescribed and monitored by a doctor — the oral form in particular requires ruling out contraindications.
In-clinic procedures
Chemical peels: can speed up fading when the right active and concentration are used. These are part of protocols such as E-Mela.
Lasers and light: can help but demand great caution. IPL and some misused lasers risk darkening melasma through heat, with a high relapse rate. They should only be performed by an experienced doctor using settings appropriate for Asian skin.
Microneedling and PRP: studied as adjuncts, usually combined with topical actives.
What every procedure has in common: results come slowly (often 3–12 months) and always carry a relapse risk if sun protection slips.
Common mistakes that make melasma worse

Using unregulated "mixed" or "fast whitening" creams. Many contain uncontrolled corticosteroids or high-strength hydroquinone — they "whiten fast" at first, then cause thinning skin, broken capillaries, steroid-damaged skin, and a worse melasma flare.
Overusing lasers or using the wrong type. Excess heat stimulates melanocytes, making melasma darker and more widespread.
Skipping sunscreen or only applying it "when I remember".
Expecting a complete cure after one course and then dropping maintenance, leading to relapse and frustration.
Self-diagnosing, confusing melasma with freckles or post-acne marks and choosing the wrong approach.
Melasma myths and facts
"Treat melasma once and it’s gone forever." → False. Melasma is chronic; the goal is control and maintenance.
"If I already have melasma, I don’t need sunscreen." → False. Skipping sun protection is the number-one reason melasma darkens and returns.
"Lasers always clear melasma." → False. The wrong laser can make melasma worse; not every case should be lasered.
"The faster a cream whitens, the better." → False and dangerous. Abnormally fast whitening usually signals corticosteroids/mixed creams.
"Melasma is caused only by the sun." → Incomplete. Sun is the biggest factor, but genetics and hormones matter too.
Can melasma be cured completely?
The honest answer: melasma usually cannot be "cured permanently," but it can be controlled well and faded significantly with the right, consistent treatment.
How much it improves depends on the type (epidermal responds better than dermal), how long you’ve had it, and — most importantly — adherence to sun protection and maintenance. The people who succeed most are those who accept this as a long-term journey, not a "quick fix".
At-home care and preventing relapse
Apply broad-spectrum sunscreen every day, even indoors near windows or with heavy screen use.
Use gentle products; avoid harsh scrubbing and irritating steps (inflammation worsens melasma).
Maintain lightening actives as directed by your doctor; don’t increase the dose on your own.
Avoid unregulated creams of unknown origin.
Return for periodic reviews to adjust the protocol — melasma changes with the seasons and hormones.
Melasma treatment at Eternal Beauty Center, Go Vap

At Eternal Beauty Center (Go Vap, Ho Chi Minh City), melasma is approached as diagnose first, personalize the protocol second. The doctor assesses the skin to identify the melasma type and pigment depth, then builds a plan combining topical actives, medical peels, and proper sun protection.
For persistent, treatment-resistant cheek melasma, the E-Mela protocol is designed specifically for difficult cases. If your concern is more about post-acne marks than true melasma, Mela Peel is a better fit — and telling them apart is exactly what the doctor does during your visit.
👉 Book a skin assessment and consultation with Dr. Le Hien to find out exactly which type of melasma you have and the right plan for it.
Frequently asked questions
How are melasma and freckles different?
Melasma is symmetrical brown/grey-brown patches with soft borders, linked to hormones and sun. Freckles are small, separate spots with a genetic basis, usually present since childhood.
Will melasma after pregnancy go away on its own?
Some pregnancy-related melasma fades after birth as hormones settle, but many cases persist and need treatment. Early sun protection helps limit worsening.
Should I get laser treatment for melasma?
Not every case should be lasered. The wrong laser can worsen melasma. A doctor must assess the type first.
How long until I see results?
Usually 3 to 12 months depending on the type and protocol. Melasma is a long journey with no safe “instant” solution.
Are anti-melasma “mixed” creams harmful?
Yes. Many contain uncontrolled corticosteroids/hydroquinone, causing thinning skin, broken capillaries, steroid damage, and a worse melasma flare over time.
What should my skincare focus on while I have melasma?
Keep it gentle, apply broad-spectrum sunscreen daily, and avoid irritating steps. Any strong lightening active should be doctor-directed.
Summary
Melasma is a chronic form of hyperpigmentation driven by overlapping factors — genetics, hormones, UV, and visible light. Telling melasma apart from freckles and post-acne marks, and identifying its type (epidermal, dermal, mixed), determines how well treatment will work.
Medical treatment always rests on sun protection as the foundation, combined with topicals (supervised hydroquinone, triple combination, azelaic acid, tranexamic acid…) and appropriate procedures such as medical peels, while lasers require great caution. Melasma rarely "clears forever," but it can be well controlled with the right, consistent treatment.
Most important of all: avoid mixed creams, don’t self-diagnose, and start with a skin assessment by a dermatologist.
Written by Dr. Le Hien — Eternal Beauty Center, Go Vap, Ho Chi Minh City. Informed by reputable dermatology sources (AAD, Mayo Clinic, DermNet, PubMed reviews). For information only; it does not replace an in-person consultation.