
Atrophic acne scars (depressed or "pitted" scars) are indentations in the skin that form when inflammation — usually from acne — destroys collagen in the dermis and the body doesn't rebuild enough to replace it. Because they are fundamentally a loss of tissue, atrophic scars do not fill in on their own over time and cannot be "cured" with a cream. The good news: modern dermatology offers several methods that deliver significant improvement — filling in most of the depression — when matched to the right scar type and performed with proper technique.
This article is a comprehensive pillar guide to atrophic scars: what they are, how they differ from raised scars and dark marks, why they form, the types, and — most importantly — a full map of treatment options, with each method matched to the scar type it works on according to medical evidence. It draws on guidance from the American Academy of Dermatology (AAD), DermNet, systematic reviews on the U.S. National Library of Medicine (NCBI/PMC) and Frontiers in Medicine, combined with real treatment experience at Eternal Beauty Center, a skincare clinic in Go Vap, Ho Chi Minh City.
What are atrophic acne scars?
Atrophic scars are scars that sit below the surrounding skin surface, forming when the healing process after an inflammatory injury fails to produce enough collagen to fill the area of destroyed tissue. In medical terms these are atrophic scars — "atrophic" meaning the tissue is deficient, shrunken.
The most common cause is inflammatory acne (pustules, nodules, cysts). Chickenpox, some skin infections, and trauma can also leave atrophic scars. According to dermatology reviews, roughly 80–90% of acne scars are atrophic (depressed) scars linked to collagen loss; a smaller share are raised hypertrophic or keloid scars.
The key point to grasp right away: an atrophic scar is a problem of the skin's structure and depth, not its color. That's why no cream, serum or "scar-treatment ointment" can "fill in" a depression — they can't rebuild the collagen lost deep in the skin. Genuine improvement always requires medical procedures that act on the dermis to stimulate or restructure collagen.
Atrophic scars, raised scars and hyperpigmentation: don't confuse them
This is the most common mix-up that sends people down the wrong treatment path for a long time. Three completely different things:
| Feature | Atrophic scar (depressed) | Raised / hypertrophic scar | Post-acne dark marks (PIH) |
|---|---|---|---|
| Nature | Indented, collagen loss | Raised, excess collagen | Only a change in color |
| To the touch | Depressed, uneven | Firm, raised | Flat skin, only different color |
| Fades on its own? | No — permanent without intervention | No | Can fade over months/years |
| How it's treated | Dermal-remodeling procedures | Entirely different (steroid injection, vascular laser…) | Sun protection + brightening actives, peels |
Post-inflammatory hyperpigmentation (PIH) is only color: the skin is flat, not depressed, just darker than the surrounding area because of increased melanin during healing. PIH can fade over months to years and responds well to sun protection, brightening actives and peels. If you're unsure whether yours is a scar or a mark, Why do you get dark marks after acne? explains the PIH mechanism; for stubborn patches, the Mela Peel treatment is designed specifically for post-acne pigmentation.
A simple at-home check: view the skin under side lighting (a lamp angled from one side). Atrophic scars cast a shadow because they're depressed; dark marks don't because the surface is flat. That's the first step in telling them apart — but identifying the exact type of atrophic scar and the right protocol still requires an in-person exam by a dermatologist.
The rest of this article focuses on atrophic scars — the hardest to treat and the most misunderstood.
Why do atrophic scars form? The collagen-loss mechanism
Understanding the mechanism explains why treating these scars is difficult and why prevention matters so much.
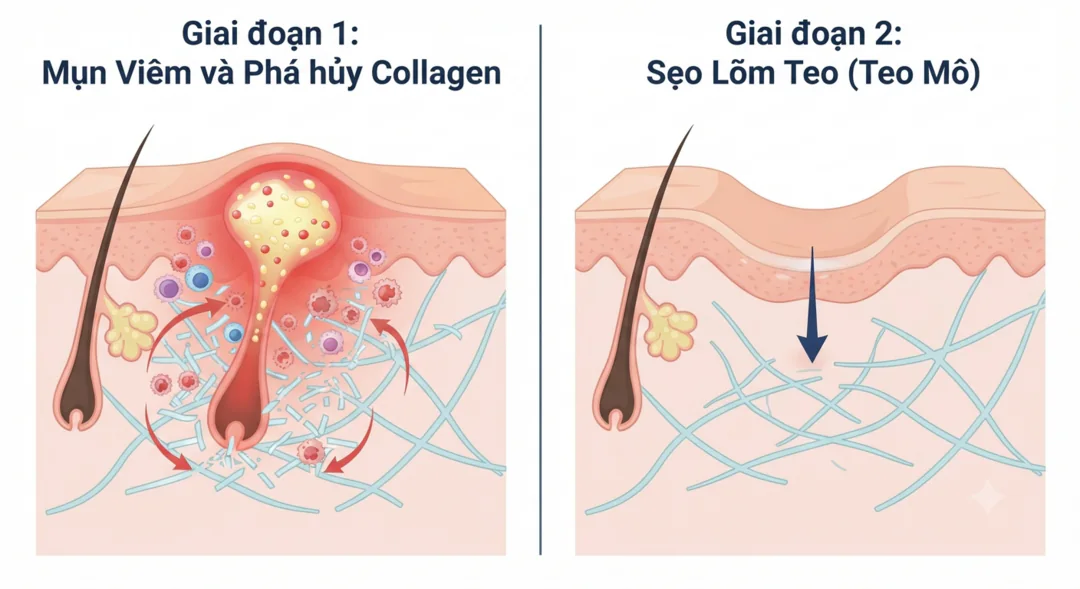
When an inflammatory pimple (especially a nodule or cyst) forms, the inflammation reaches down into the dermis — the layer holding most of the collagen and elastin that support the skin's structure. If the inflammation is strong or prolonged enough, it destroys the collagen bundles there. During healing, the body tries to repair, but:
If it produces too little collagen relative to what was lost → the skin sinks → atrophic (depressed) scar.
If it produces too much collagen → tissue rises → hypertrophic/keloid scar.
In addition, fibrous bands can form, tethering the scar base down to the underlying tissue — creating a fixed "rolling" depression.
Three factors raise the risk of atrophic scarring:
Degree of inflammation: deep inflammatory acne (nodules, cysts) scars more readily than surface blackheads or whiteheads.
Time: the longer inflammatory acne goes uncontrolled, the more tissue is destroyed.
Mechanical trauma: improper picking, squeezing or popping pushes inflammation deeper and breaks down skin structure — one of the most common and most avoidable causes of atrophic scarring.
Because deep collagen does not regenerate in exactly the place it was lost, atrophic scars are permanent without intervention. Every effective treatment centers on one goal: stimulating the body to make new collagen at the depressed area, cutting the fibrous bands tethering the scar base, or resurfacing the top layer.
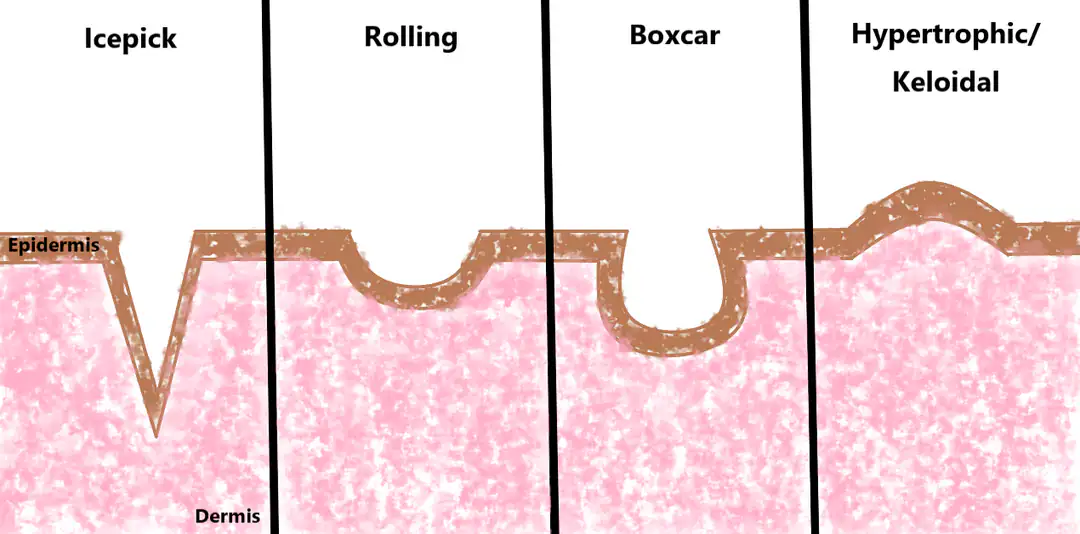
The three types: ice pick, boxcar, rolling
Dermatology classifies atrophic scars into three main types based on shape and depth. Correct classification determines the treatment — which is why two people with "acne scars" can need completely different protocols.
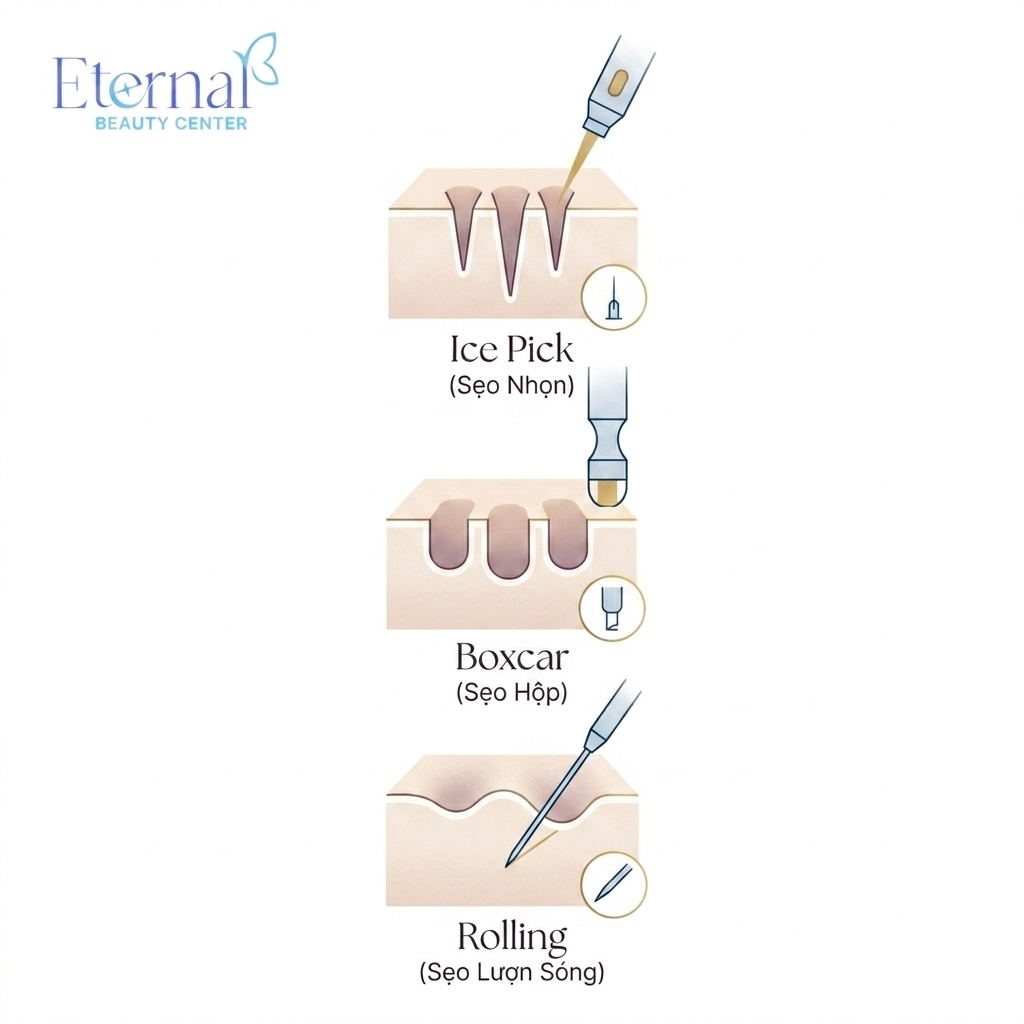
Ice pick scars: narrow (usually under 2mm), deep and pointed as if punctured, reaching deep into the dermis. This is the hardest type to treat because the base is so deep and narrow.
Boxcar scars: wider, with sharply defined vertical edges and a flat base — like a round or oval "crater." They come in shallow and deep varieties.
Rolling scars: wide, with sloping edges, giving the skin surface a "wavy," undulating look. Usually caused by fibrous bands tethering the base down.
In practice, most people have several types coexisting on the same face — for example ice pick on the cheeks, boxcar on the temples, rolling on the cheekbones — so protocols usually combine multiple techniques.
This article summarizes the types so you have the big picture. For a deep dive into how to identify each type precisely and why each needs its own approach, read the dedicated article: Distinguishing the 3 types of acne scars — and why each needs a different approach.
Do atrophic scars fill in on their own?
The short answer: no. Because an atrophic scar results from lost collagen in the dermis, and lost collagen doesn't regenerate in place, the depression remains permanently without medical intervention. Skin may look better as an accompanying red mark fades, but the depression itself doesn't change.
This also explains why topical "scar-treatment" creams and serums can't fill in the depression: most topical actives only reach the shallow epidermis, not the deep collagen damage. Some actives (retinoids, vitamin C, sunscreen) play a supporting role — improving surface texture, fading accompanying marks, and most importantly preventing new acne from creating more scars — but they don't replace dermal-remodeling procedures.
If you're thinking "let me try at home first," Can atrophic scars be treated at home? explains in detail what home skincare can and can't do, and when scars genuinely need a medical approach.
A map of atrophic scar treatments
This is the core. There's no "magic method" for every scar — each technique has its own mechanism and the scar type it's best at. The table below summarizes suitability by medical evidence; the sections that follow explain each method.
| Method | Ice pick | Boxcar | Rolling | Main mechanism |
|---|---|---|---|---|
| TCA CROSS | ⭐ Best | Fair (deep) | Rarely used | Collagen remodeling at the scar base |
| Subcision | Poor alone | Poor alone | ⭐ Best | Cuts tethering fibrous bands |
| Microneedling | Poor | Fair (shallow) | Good | Broad-area collagen stimulation |
| RF microneedling | Moderate | Good | Good | RF heat + needles, safer for dark skin |
| Fractional CO2 laser | Moderate | Good | Good | Resurfacing + collagen |
| Punch excision / elevation | Good (deep) | Good (deep boxcar) | – | Mechanically removes/raises the base |
| Dermal fillers | Minimal | Fair (temporary) | Good (temporary) | Mechanically lifts the base instantly |
6.1. TCA CROSS — the "key" for ice pick scars
TCA CROSS (Chemical Reconstruction of Skin Scars) spots high-concentration trichloroacetic acid (50–100%) precisely into the base of each ice pick scar. The acid creates a controlled injury at the scar base, stimulating collagen remodeling that gradually makes the scar shallower and narrower. This gives the most consistent, best results for ice pick scars — a type that resists other techniques. It requires multiple sessions (usually 4–6 weeks apart), and the degree of improvement correlates with TCA concentration and number of sessions.
6.2. Subcision — for rolling scars
Subcision uses a special needle tip (a sharp Nokor needle, or a blunt cannula) threaded under the skin to cut the fibrous bands tethering the scar base to the layer below. Once the bands are released, the base lifts and the healing process stimulates new collagen to fill it in. Subcision is the most effective option for rolling scars, while it's almost ineffective if used alone for ice pick or boxcar scars — because those aren't tethered by bands. A blunt cannula suits broad areas and causes less bruising than a sharp needle.
6.3. Microneedling — the broad-area foundation
Medical microneedling creates thousands of tiny micro-injuries with needle tips, stimulating broad-area collagen production. It's a good foundation for rolling and shallow boxcar scars, but poor for ice pick scars and scars with deep fibrous bands (the needles can't release the bands). Note the difference between medical microneedling (sterile needles, controlled depth, performed at a professional clinic) and an at-home dermaroller — which isn't deep enough, risks infection, and can make things worse.
6.4. RF microneedling — preferred for Asian skin
RF microneedling combines needles with radiofrequency (RF) energy delivering heat at the needle tips, stimulating deep collagen remodeling while affecting the skin surface less. That characteristic makes RF microneedling preferred for darker skin (Fitzpatrick III–V, like most Vietnamese skin), because the risk of post-inflammatory hyperpigmentation (PIH) is lower than with ablative lasers. It works well on boxcar and rolling scars.
6.5. Fractional CO2 laser — the "gold standard" for resurfacing
Fractional CO2 laser (10,600nm) creates columns of micro-thermal injury through the skin, both resurfacing the top layer and stimulating deep collagen — considered a "gold standard" for scar resurfacing, effective on boxcar and rolling scars. The trade-off: CO2 laser has longer downtime and a higher PIH risk on darker skin, so parameters and pre/post care must be carefully considered for Asian skin. At reputable clinics, devices are chosen from FDA-cleared makers (e.g. Lutronic, Deka).
6.6. Punch techniques and dermal fillers
For certain deep, isolated ice pick or boxcar scars, a doctor may use punch techniques (excising or elevating the scar base) to mechanically remove the scar and let the skin heal flatter. Dermal fillers — usually hyaluronic acid — can lift the base of rolling/boxcar scars for instant but temporary results (lasting months to over a year depending on type), often used in combination or to "preview" the result. Fillers are minimally effective for ice pick scars.
6.7. Peels and supportive care
For very shallow scars, or to smooth surface texture and address accompanying marks, chemical peels (salicylic/TCA at appropriate strengths) may be combined — but peels cannot fill deep scars, so they're rarely used alone for atrophic scarring. To understand what a peel really is, see What is a chemical peel. Alongside this, barrier-repair steps and restorative growth-factor serums (EGF booster) before and after procedures help the skin heal better and reduce complications.
Why there's no "one method for everything"
If there's one message to take from this article, it's this: effective atrophic scar treatment is almost always combined and personalized. Medical reviews agree on one point: "there is no panacea for atrophic scars" — because each type has a different mechanism, and most faces carry several scar types at once.
A realistic protocol often looks like this: subcision releases fibrous bands in the rolling-scar zones, TCA CROSS spot-treats each ice pick scar, microneedling or RF microneedling provides broad-area collagen stimulation, and recovery care sits between sessions. Deciding which technique goes where, in what order, and how far apart — that's the clinical judgment only a dermatologist assessing you in person can make.
This is also why you should be wary of anywhere advertising "one technology for all scar types" or "scar-free after one session." Atrophic scars need a course of treatment, not a single visit.
Timeline and realistic expectations
Setting the right expectations is the foundation of satisfaction. A few practical principles:
The goal is "improvement," not "100% gone." With the right protocol, most people improve markedly — many scars fill in around 70–90% — but "perfectly smooth as if there were never a scar" is not what medicine promises. The degree of improvement depends on scar type, depth, individual biology and adherence.
It takes multiple sessions, weeks apart. The skin needs time to make new collagen between sessions; techniques like TCA CROSS, microneedling and subcision are typically repeated several times, 4–6 weeks apart. Results come gradually over months.
Asian skin needs to watch for PIH. Fitzpatrick III–V skin is prone to post-inflammatory hyperpigmentation; so choosing the method (e.g. favoring RF microneedling over CO2 laser where appropriate), tuning parameters and strict sun protection after procedures are mandatory to avoid post-treatment darkening.
Older scars aren't hopeless. Scars 5+ years old often still improve well after a combined protocol — because these techniques act on structure, independent of the scar's "age."
You can see a real example of an acne–pigmentation–scar journey in this treatment case file at Eternal (results vary by individual).
Preventing scars: treating acne early is the key
The best way to "treat atrophic scars" is to stop them from forming. Because atrophic scars start from inflammatory acne destroying collagen, controlling acne early and correctly is the most effective prevention:
Treat inflammatory acne early, with the right protocol — don't wait for it to "clear on its own." The longer nodules and cysts persist, the more likely they scar. See medical-grade acne treatment (E-Acne) or the overview everything you need to know about acne.
Don't pick, squeeze or pop. This is the most avoidable cause of atrophic scarring. If extractions are needed, have a professional do them properly — see the medical-grade acne extraction protocol.
Protect from the sun and don't peel scabs while the skin heals, to limit both scars and marks.
Put simply: investing in acne control today is far cheaper and less painful than treating atrophic scars later.
Atrophic scar treatment at Eternal Beauty Center

At Eternal Beauty Center (Go Vap, Ho Chi Minh City), atrophic scars are treated exactly in the spirit of this article — personalized, multimodal, technique chosen by scar type and skin tone — not chasing "one technology for all":
E-Scar – Medical-grade atrophic scar treatment: a protocol designed individually after a dermatologist (Dr. Le Hien) examines and classifies the scars in person, combining the appropriate techniques: TCA CROSS (ice pick scars), subcision with Nokor needle/cannula (rolling scars), microneedling and RF microneedling (collagen stimulation, with RF microneedling favored for pigmentation-prone skin), fractional CO2 laser where appropriate, plus restorative care between sessions.
Transparent commitment: after the skin analysis and exam, the doctor gives an honest forecast of the improvement and number of sessions needed; the cost is quoted clearly upfront per protocol (direct consultation via hotline/Zalo).
Realistic expectations: we don't promise "100% scar-free after one session" — medicine doesn't allow such a promise. What we commit to is marked improvement, safe for your skin tone, on a plan agreed in advance — done properly.
If you're not sure which type your scars are or what protocol you need, the first step is always an accurate exam and classification with a doctor.
Frequently Asked Questions (FAQ)
Do atrophic acne scars fill in on their own?
No. Atrophic scars result from collagen loss in the dermis, and lost collagen doesn't regenerate in place. The depression is permanent without medical intervention. Topical creams can't fill deep scars; genuine improvement requires dermal-remodeling procedures such as TCA CROSS, subcision, microneedling, RF microneedling or laser.
How do I tell an atrophic scar from a dark mark?
An atrophic scar is a depression (a structural change, collagen loss) and casts a shadow under side lighting. Post-acne hyperpigmentation (PIH) is only color — flat skin, darker than surroundings — and can fade over months/years. The two need different treatments; many people treat the wrong thing because they confuse them.
How many types of atrophic scars are there?
Three main types: ice pick (narrow and deep), boxcar (wide with steep edges), and rolling (wide with sloping edges). Each needs a different method, and most people have several types at once, so protocols usually combine techniques.
Which method is best for atrophic scars?
There's no single "best" for all types. TCA CROSS is best for ice pick; subcision is best for rolling; microneedling, RF microneedling and CO2 laser suit boxcar and rolling. So effective treatment is almost always a combination, personalized by a doctor to your scar types and skin tone.
How many sessions does atrophic scar treatment take?
It depends on scar type, depth and individual factors, but it almost always requires multiple sessions 4–6 weeks apart, because the skin needs time to build new collagen between sessions. Results come gradually over months. The exact number is only clear after a doctor examines and classifies the scars.
Can scar treatment cause dark marks?
It can, if the method and aftercare aren't right. Vietnamese skin (Fitzpatrick III–V) is prone to post-inflammatory hyperpigmentation, so in many cases RF microneedling is favored over ablative laser to lower the risk; strict sun protection after procedures is mandatory. Done with proper technique, the risk is well controlled.
Can old scars (5–10 years) still be treated?
Yes. Scar-treatment techniques act on the skin's structure (fibrous bands, scar base, collagen), independent of the scar's "age." Many years-old scars still improve well after a combined protocol. What matters is correctly assessing the scar type and following the plan.
Should I use an at-home dermaroller on scars?
No. At-home dermarollers usually aren't deep enough to affect scars, risk infection and irritation, and can make things worse. Medical microneedling needs sterile needles, controlled depth and a professional setting. See the analysis in can atrophic scars be treated at home.
Summary
Atrophic scars are depressions caused by collagen loss in the dermis — a structural problem, not a color one — so they don't fill in on their own and can't be treated with creams. The most important takeaways:
Clearly distinguish atrophic scars (depressed) — raised scars — dark marks (color only): three conditions, three different treatments.
Atrophic scars come in three types — ice pick, boxcar, rolling — each with its own best method.
There's no "one method for everything": effective treatment is almost always combined and personalized — TCA CROSS for ice pick, subcision for rolling, microneedling/RF microneedling/laser as the foundation.
The right expectation is marked improvement (often 70–90%), across several sessions, not "100% gone after one visit."
Vietnamese skin should mind the risk of post-treatment darkening — choose the right method and protect from the sun rigorously.
The best way to prevent scars is to control acne early and never pick at it.
Book a skin analysis & atrophic scar consultation at Eternal Beauty Center
Not sure which type your scars are, or tried treatment before without improvement? A dermatologist at Eternal Beauty Center will analyze your skin, classify the scars and recommend a personalized protocol — with an honest forecast of the improvement and number of sessions.
Hotline / Zalo: 0334 713 610
Address: 204 Street No. 1, Ward 16, Go Vap, Ho Chi Minh City
Opening hours: 10:00 – 20:00 daily
Related: E-Scar – Medical-grade scar treatment · Distinguishing the 3 types of acne scars · Can atrophic scars be treated at home
Medical disclaimer: This article is for informational purposes only and does not replace an in-person examination, diagnosis or personalized medical advice. Atrophic scar treatment is a procedure that must be indicated and performed by a qualified doctor; effectiveness and suitability vary between individuals depending on scar type, skin tone and biology. Please consult a dermatologist before undergoing treatment.


