
Acne (medically, acne vulgaris) is a chronic inflammatory disease of the pilosebaceous unit — the hair follicle and its oil gland — that develops when four factors coincide: excess sebum, follicular clogging from abnormal keratinization, growth of the bacterium Cutibacterium acnes, and inflammation. It is the single most common skin condition: according to the American Academy of Dermatology (AAD), acne affects nearly 50 million people a year in the United States alone, and up to 85% of adolescents experience it. Acne is not life-threatening, but left uncontrolled it can leave permanent dark marks and atrophic scars — and it takes a real toll on confidence and mental well-being.
This is a pillar guide to acne: what acne is and why it forms at the mechanistic level, how many types exist and how to tell the confusable ones apart (hidden acne, inflammatory acne, hormonal acne, dark marks, scars), the real evidence-based causes, and — most importantly — the medical-grade treatment ladder from topicals to oral medication to in-clinic procedures. It draws on AAD, DermNet, StatPearls (NCBI), and review articles in the U.S. National Library of Medicine (PMC), combined with real-world treatment experience at Eternal Beauty Center, a skin clinic in Go Vap District, Ho Chi Minh City.
What is acne?
Acne vulgaris is a chronic skin disease of the pilosebaceous unit — a structure made up of a hair follicle and its attached oil (sebaceous) gland, most densely located on the face, neck, chest, shoulders, and back. In healthy skin, the gland secretes just enough oil to moisturize and protect. When that unit malfunctions — excess oil, dead cells, and bacteria clogging the pore — acne lesions appear.
A few numbers show how common it is:
Acne is the most common skin disease of all. According to StatPearls (NCBI), up to 70% of people experience acne at some point in life.
The AAD reports that acne affects nearly 50 million Americans a year and up to 85% of people aged 12–24.
Acne is not only a teenage problem: adult acne is rising, affects about 15% of women, and can persist into — or newly appear in — one's 30s and 40s.
Roughly 10% of cases progress to severe nodulocystic acne, which carries a real risk of permanent scarring.
The key point to grasp up front: acne is a disease with a defined mechanism, not "dirty skin" or poor hygiene. Because it has a mechanism, acne is treatable — but it needs the right approach, the right targets, and patience, not simply waiting for it to "go away on its own."
How acne forms: the four factors
Understanding the mechanism is the key to understanding why acne keeps coming back and why each treatment targets a different link in the chain. The medical literature agrees that acne forms from four factors acting together inside the pilosebaceous unit:
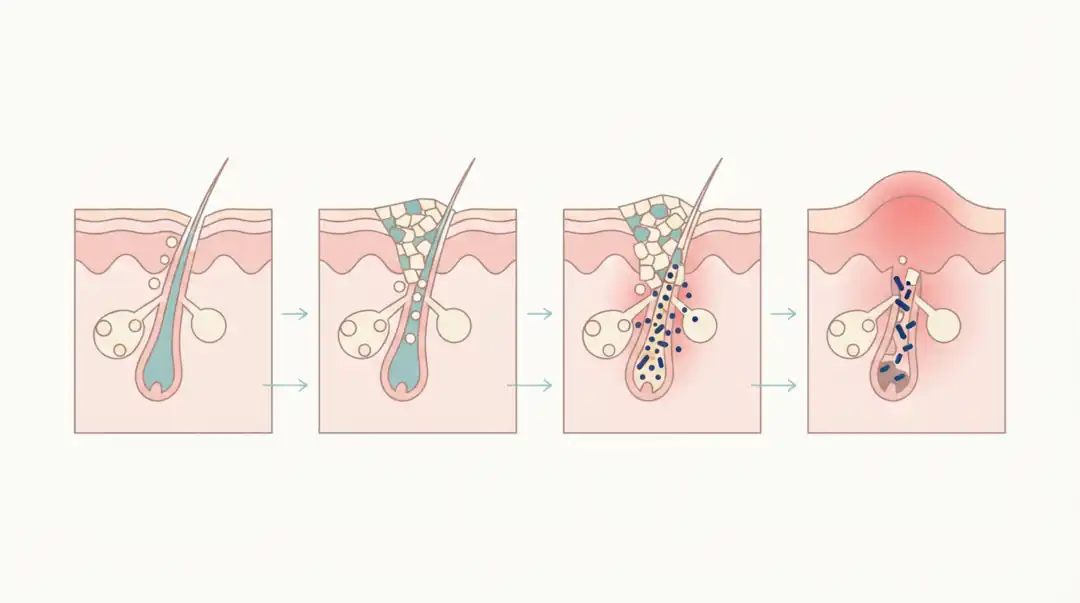
1. Excess sebum (too much oil). Driven by androgen hormones, the oil gland works harder and secretes more sebum, creating an environment that favors acne. This is why acne peaks in puberty and around the menstrual cycle. 2. Follicular hyperkeratinization (clogging). Dead cells at the follicle opening fail to shed normally and stick together, sealing the pore. Trapped oil and dead cells form a microcomedone — the "seed" of every acne lesion. 3. The bacterium Cutibacterium acnes. This normal skin resident (renamed from Propionibacterium acnes in 2016) multiplies in the clogged, oil-rich environment and triggers inflammation. 4. Inflammation. The immune system reacts to the bacteria and their metabolites, causing swelling, redness, and pain — turning a "silent" comedone into a visible inflammatory lesion.
Every acne lesion begins as a microcomedone. If the plug stays sealed under the skin → a whitehead (hidden acne); if it opens and oxidizes → a blackhead; if inflammation sets in → papules, pustules, and in worse cases nodules and cysts. This is precisely why an effective acne regimen must address several factors at once — reduce oil, unclog follicles, control bacteria, and calm inflammation — rather than relying on a single ingredient.
Types of acne: non-inflammatory and inflammatory
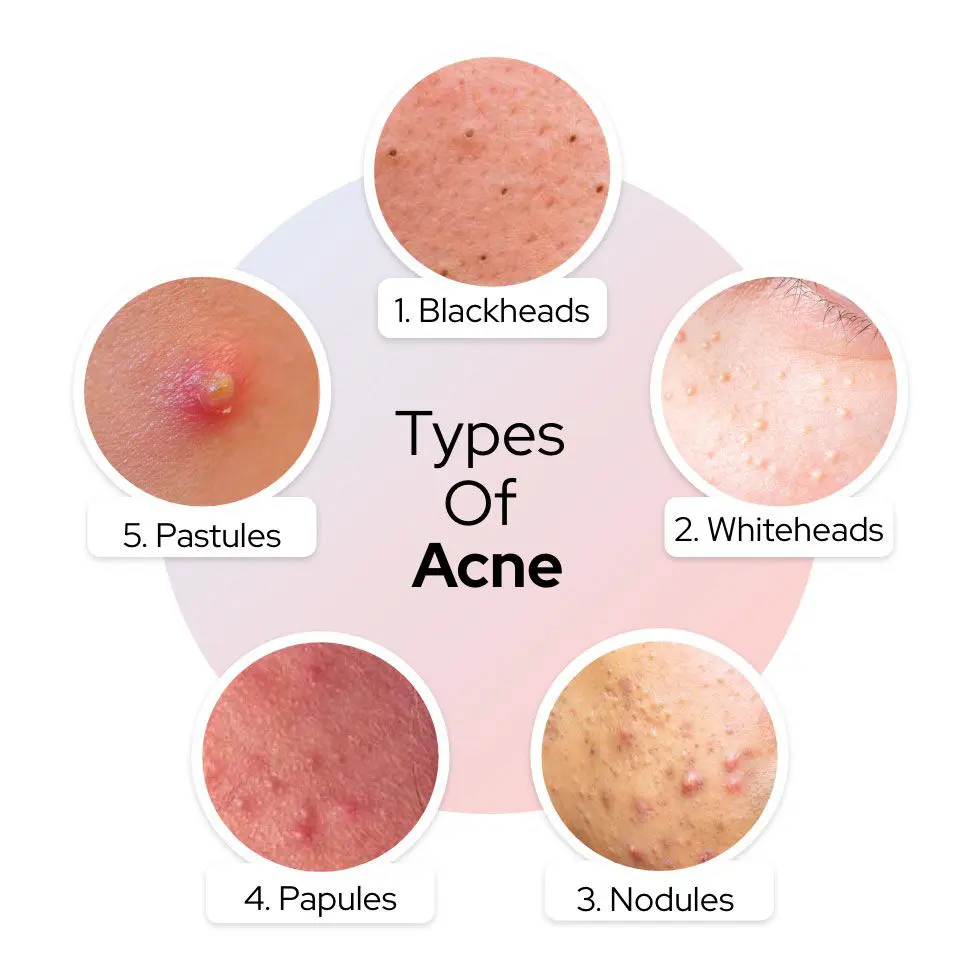
During a single flare, skin usually shows several types of acne at once. Correctly identifying the type is the first step to choosing the right approach. The literature divides acne into two broad groups: non-inflammatory (comedones) and inflammatory.
| Acne type | Group | How to recognize it |
|---|---|---|
| Blackhead (open comedone) | Non-inflammatory | Open plug, dark tip from sebum oxidizing in air — not from dirt |
| Whitehead / hidden acne (closed comedone) | Non-inflammatory | Small sealed bump under the skin, white or skin-colored, feels rough |
| Papule | Inflammatory | Small red raised bump 2–5 mm, no pus, slightly tender |
| Pustule | Inflammatory | Red bump with a white or yellow pus head |
| Nodule | Severe inflammatory | Hard, painful mass deep under the skin, usually >5 mm |
| Cyst | Severe inflammatory | Large pus-filled sac, soft, prone to leaving scars |
Knowing the group points you in the right direction: non-inflammatory acne (blackheads, hidden acne) mainly needs unclogging and normalized keratinization; inflammatory acne (papules, pustules, nodules, cysts) additionally needs bacterial control and anti-inflammatory action — and the deeper the inflammation, the higher the scarring risk, so early, correct intervention matters.
Hidden acne in particular confuses many people because it sits deep, lingers, and recurs easily. If this is your problem, the deep-dives Does hidden acne go away on its own? and popular methods for clearing hidden acne analyze the right way to handle it. For a quick overview of acne types and warning signs, see Everything you need to know about acne.
Severity grading: why it decides the protocol
It is not the type of acne but the severity that decides the treatment protocol. Dermatologists usually grade acne into three levels based on the number and depth of lesions:
| Severity | Features | Treatment direction |
|---|---|---|
| Mild | Mostly comedones (blackheads, whiteheads), a few papules/pustules, no nodules or cysts | Usually responds to topicals + correct care |
| Moderate | Many comedones plus clearly inflamed papules and pustules | Usually needs topical + oral and/or supportive procedures |
| Severe (nodulocystic) | Multiple large nodules and cysts >5 mm, painful, scarring often present | Needs active medical intervention, consider isotretinoin; prioritize scar prevention |
Why does this matter? Because the same word "acne" can require completely different protocols in two people. Someone with mild acne may improve on a topical retinoid and sunscreen alone; someone with nodulocystic acne treated too gently will keep accumulating scars with every passing day. This is why a proper exam to classify and grade is always the first step before choosing a method — rather than buying products off an advertisement.
Easily confused: hidden acne, hormonal acne, dark marks, and scars
Many people treat the wrong problem for a long time simply because they confuse these concepts. Here are the most important distinctions.
Hidden acne vs inflammatory acne. Hidden acne (whiteheads) is a non-inflammatory comedone sealed under the skin — no redness or swelling; it is essentially a clogged follicle. Inflammatory acne (papules, pustules, nodules) is when that comedone has become inflamed — swollen, red, painful. Hidden acne easily turns inflammatory when provoked (bad squeezing, pore-clogging products).
Hormonal acne. This is not a separate lesion type but acne driven by androgen hormones, typically showing as deep inflammatory lesions on the chin, jawline, and around the mouth, worsening with the menstrual cycle and lingering in adult women. Hormonal acne often responds poorly to topicals alone and may need hormonal treatment (e.g. anti-androgen medication) assessed by a doctor.
Acne vs dark marks vs scars — three completely different problems needing different solutions:
| Feature | Active acne | Post-acne dark marks (PIH) | Atrophic scars |
|---|---|---|---|
| Nature | Inflamed lesion / clogged follicle | Only a color change | Loss of collagen, a depression |
| To the touch | Raised, swollen, has a core | Skin is flat, only differs in color | Has a depression, uneven surface |
| Resolves on its own? | Possibly, if the cause is controlled | Can fade over months/years | No — permanent without intervention |
| Approach | Treat the acne (Section 7) | Sunscreen + brightening actives, peels | Dermal remodeling procedures |
A quick at-home check: examine skin under side lighting. Atrophic scars cast a shadow because they are indented; dark marks cast no shadow because the surface is flat. If a dark patch remains after a pimple heals, Why do dark marks linger after a pimple has healed? explains post-acne pigmentation and how to handle it; for stubborn marks, the Mela Peel protocol is designed for post-acne hyperpigmentation. If it is a depression, read the guide What are atrophic acne scars and how are they treated — because scars need a completely different approach.
Causes and aggravating factors
Acne is a multifactorial disease. The foundation is the four-factor mechanism in Section 2, but many internal and external factors can "light the fuse" or make acne worse:
Hormones (androgens). This is the main driver. Androgens stimulate the oil gland to produce more sebum, which is why acne flares in puberty, around menstruation, during pregnancy, or in polycystic ovary syndrome (PCOS).
Genetics. If parents had severe acne, a child's risk and severity are often higher.
Diet. The strongest evidence links high-glycemic foods (sweets, refined carbs) to worse acne — they raise insulin and IGF-1, which indirectly increase sebum and comedone formation. For dairy, evidence is less consistent, though some studies suggest it can worsen acne in sensitive people. By contrast, "chocolate causes acne" is not clearly proven by science.
Cosmetics and pore-clogging products. Comedogenic creams, makeup, or oils can trigger acne — including the "purge" when switching to a new product. See how to avoid breakouts when using new cosmetics.
Friction and mechanical pressure. Pressing and rubbing (masks, helmets, resting your chin on your hand) and especially improper squeezing, picking, and popping push inflammation deeper, worsen acne, and raise the risk of scarring.
Stress and sleep. They don't directly "create" acne but disrupt hormones and make acne harder to control.
Hot, humid climate. In Vietnam, sweat and high humidity make skin oilier, so acne flares more easily and post-acne marks are darker — making early care especially important.
The point worth stressing: acne is not caused by poor hygiene. Over-washing or scrubbing harshly actually damages the skin barrier and makes acne worse.
The medical-grade treatment ladder

This is the core section. Per the AAD's 2024 guidelines, effective acne treatment is combination therapy targeting multiple mechanisms, chosen by severity, and prioritizing reduced antibiotic resistance. Think of it as a "ladder" from mild to severe.
1. Topicals (the backbone of every protocol)
Topical retinoids (tretinoin, adapalene, tazarotene, trifarotene): normalize keratinization, unclog follicles, and reduce comedone formation — the backbone of acne care. The AAD notes no single retinoid is definitively superior to another.
Benzoyl peroxide (BPO): kills C. acnes, reduces inflammation, and lowers resistance risk when paired with antibiotics.
Topical antibiotics (clindamycin, erythromycin): reduce inflammation and bacteria — best used with BPO, not alone long-term, to avoid resistance.
Azelaic acid, salicylic acid (BHA), clascoterone: supportive options for comedones, mild inflammation, and post-acne marks.
2. Oral medication (for moderate–severe or hormonal acne)
Oral antibiotics (doxycycline is strongly recommended; minocycline, sarecycline): used short-term, always with topicals (BPO/retinoid), never long-term alone.
Hormonal therapy for women: combined oral contraceptives and spironolactone (anti-androgen) — especially effective for hormonal acne on the chin and jawline in adult women.
Oral isotretinoin: strongly recommended for severe acne, scarring acne, acne causing psychosocial distress, or acne failing standard therapy. Highly effective, but it requires a physician's prescription and close monitoring because of significant side effects and contraindications (notably pregnancy).
Isotretinoin is neither "the only lifeline" nor "a drug to avoid at all costs." A real story of treating stubborn acne without relying on isotretinoin is told in A 9-year acne treatment journey — illustrating why protocols must be individualized.
3. Supportive in-clinic procedures
Medical-grade extraction: removing comedones, blackheads, and hidden acne with sterile technique at the right time — keeping skin clear and reducing the risk of a ruptured core causing inflammation. This is a major difference from squeezing at home; see the medical-grade acne extraction process.
Chemical peels: AHA/BHA/retinoid at appropriate strengths speed up cell turnover, unclog follicles, and improve marks. To understand the fundamentals, see What is a chemical peel.
Light, laser, and supportive technologies: help reduce inflammation and oil in select cases, always alongside the main protocol.
The golden rule: no single product or technology "treats every kind of acne." A good protocol combines topical, oral, and procedural treatment at the right level, adjusted to how the skin responds, and always includes sun protection to limit dark marks.
Common myths about acne
Many false beliefs make acne worse. Some of the most common:
"Blackheads are dirt." False. The dark color comes from sebum and keratin oxidizing in air, not dirt. Scrubbing hard to "clean" only irritates.
"The more you wash, the clearer you'll get." False. Over-washing damages the barrier, dehydrates skin, and can trigger more oil in compensation. Gently washing twice a day is enough.
"Just squeeze out the core and the skin is clean." False and dangerous. Improper squeezing and picking drive inflammation deeper, spread acne, and are one of the most avoidable causes of scarring.
"Acne will clear on its own — no need to treat it." Not necessarily. Some mild acne may improve, but persistent inflammatory and hidden acne usually needs intervention — and the longer you wait, the higher the risk of marks and scars. See the analysis in does hidden acne go away on its own.
"You don't need sunscreen while you have acne." False. Sun makes post-acne marks darker and slower to fade, and many acne actives make skin sun-sensitive — so sunscreen is essential.
When should you see a dermatologist?
Good at-home care can control many mild cases. However, you should see a dermatologist when:
Acne is moderate to severe, or you have nodules or cysts — the group most likely to scar.
Acne has already left marks or scars, or you see scarring beginning to form.
You've used over-the-counter products correctly for a few months with no improvement.
Acne is persistent into adulthood, concentrated on the chin and jawline, with suspected hormonal involvement.
Acne clearly affects your mental well-being, confidence, and quality of life.
Early, correct intervention not only clears skin faster but, more importantly, prevents atrophic scars — which are far harder and costlier to treat later.
Acne treatment at Eternal Beauty Center

At Eternal Beauty Center (Go Vap, HCMC), acne is handled exactly in the spirit of this article: examine, classify, and grade first, then individualize the protocol, combining topical, oral, and procedural treatment at the right level — rather than a "one protocol for everyone." A dermatologist (Dr. Le Hien) personally assesses the skin and designs the plan. Depending on the condition, treatments may be selected and combined:
E-Acne – Medical-grade acne treatment: a comprehensive acne protocol with close physician oversight, FDA-standard equipment, minimizing reliance on oral medication, and focused on preventing recurrence.
O2 Peel – Medical-grade manual extraction: softening the skin with an oxygen peel, then removing the core under sterile, physician-supervised conditions — far safer than squeezing yourself.
Acne Peel: a peel protocol tailored to acne-prone skin, using AHA/BHA/PHA/retinoid to address acne through multiple mechanisms.
Mela Peel: for post-acne dark marks (PIH) — addressing the "color" that remains after a pimple has healed.
Transparency and realistic expectations: after the skin exam, the doctor gives an honest forecast of improvement and the timeline needed; we don't promise "clear skin in one session" — treating acne is a process. You can see one real journey in the case file improving acne, dark marks, and scars at Eternal (results vary by individual).
Frequently asked questions (FAQ)
What is acne and why do people get it?
Acne (acne vulgaris) is a chronic inflammatory disease of the pilosebaceous unit. It forms when four factors coincide: excess sebum (from androgens), follicular clogging from abnormal keratinization, growth of the bacterium Cutibacterium acnes, and inflammation. So acne is a disease with a defined mechanism — not "dirty skin" — and it is treatable when those factors are targeted correctly.
How many types of acne are there?
Acne falls into two groups: non-inflammatory — blackheads (open comedones) and whiteheads/hidden acne (closed comedones); and inflammatory — papules, pustules, nodules, and cysts. All begin as a microcomedone. A flare usually shows several types at once, and it is the severity (mild, moderate, severe) that decides the treatment protocol.
Does acne go away on its own?
Some mild acne may improve, but persistent inflammatory and hidden acne usually needs proper treatment. Letting acne linger increases the risk of dark marks and atrophic scars, which are far harder and costlier to treat later. So if acne is moderate to severe, or scarring has begun, see a dermatologist early rather than waiting for it to "clear on its own."
What causes acne — is it food and dirty skin?
The foundation is the hormone–follicle–bacteria–inflammation mechanism, plus genetics. On diet, the clearest evidence is that high-glycemic foods can worsen acne; dairy's role is inconsistent; "chocolate causes acne" is not clearly proven. Acne is not caused by poor hygiene — over-washing actually makes skin worse.
What does medical-grade acne treatment involve?
Per AAD guidelines, it combines multiple mechanisms by severity: topicals (retinoids, benzoyl peroxide, topical antibiotics, azelaic/salicylic acid) as the backbone; oral medication (short-term antibiotics, hormonal therapy for women, isotretinoin for severe acne) for moderate–severe cases; and supportive procedures such as medical-grade extraction and chemical peels. The protocol must be individualized after a doctor's exam, with sun protection to limit dark marks.
Does popping pimples cause scars?
Yes. Squeezing, picking, and popping incorrectly push inflammation deeper, spread acne, and are one of the most avoidable causes of atrophic scarring. If a core needs removing, have it done at a professional clinic with sterile technique at the right time.
Do I need sunscreen while I have acne?
Very much so. Sun makes post-acne marks darker and slower to fade, and many acne actives (like retinoids) make skin sun-sensitive. Proper sun protection is a mandatory part of every acne protocol.
Key takeaways
Acne (acne vulgaris) is a chronic inflammatory disease of the pilosebaceous unit, formed by four factors: excess oil, clogging, C. acnes bacteria, and inflammation. The most important things to remember:
Acne is a disease with a mechanism, not "dirty skin" — so it is treatable when targeted correctly.
There are two groups (non-inflammatory and inflammatory), but severity decides the protocol.
Clearly distinguish acne, dark marks, and scars: three different problems, three different solutions.
Medical-grade treatment is combined topical, oral, and procedural care, individualized by severity — there is no "one protocol for everyone."
Bad squeezing and letting acne linger are avoidable causes of scarring — early intervention is the best way to protect your skin.
Book a skin exam & acne consultation at Eternal Beauty Center
Struggling with persistent acne, inflammatory breakouts, or worried about marks and scars? A dermatologist at Eternal Beauty Center will examine, classify, and grade your acne, then recommend an individualized protocol — with an honest forecast of the journey ahead.
Hotline / Zalo: 0334 713 610
Address: 204 Street No. 1, Ward 16, Go Vap District, Ho Chi Minh City
Opening hours: 10:00 – 20:00 daily
Explore our services: E-Acne – Acne treatment · O2 Peel – Extraction · Acne Peel · Mela Peel – Post-acne marks
Medical disclaimer: This article is for informational purposes and does not replace a personal exam, diagnosis, or medical advice. Acne treatment should be prescribed and monitored by a qualified physician; effectiveness and suitability vary by individual, acne type, severity, and skin. Please consult a dermatologist before starting any protocol, especially oral medication such as isotretinoin.


